
The use of medication for bipolar disorder is one of the biggest challenges in the field of psychiatry.
The untreated manic episodes tend to last 3-6 months; the untreated depressive episodes are longer, up to one year. The treatment with medication significantly reduces the duration of the episodes.
The goal of the treatment between the episodes is to extend stable periods and, in the best-case scenario, to keep the patient symptom-free for life.
For more information about bipolar disorder, contact our German Consultant in Psychiatry, Dr. Kowal
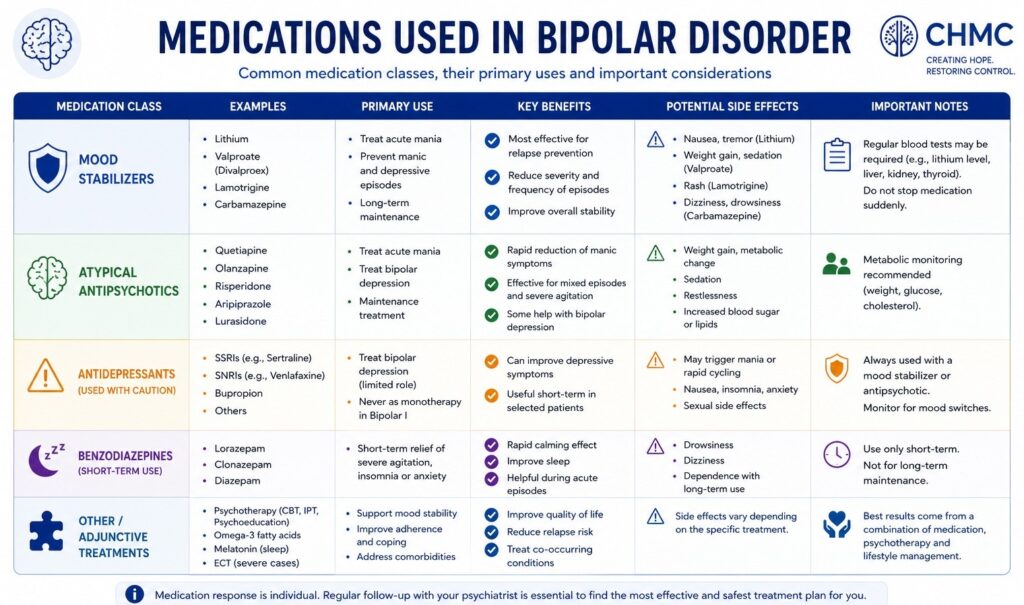
Medication for Bipolar Disorder

Some people believe that bipolar disorder can be healed with psychotherapy. The question that arises, though, is how a person can benefit from psychotherapy (counselling/talk therapy) if they are in a state of confusion, are irrational, and possibly aggressive.
During a manic episode, patients are often in denial about their condition and have no ability to gain insight. The only way to treat patients during acute mania is to use medication. In most of such cases, the psychiatrist must initially hospitalize the patient.
Medication for Manic Phase in BD
During the manic phase, the patient’s irrational behaviour can severely affect his social and economic status. The patient can overspend, buying useless but expensive items, gambling, or even donating money, which can end in a financial catastrophe or even total impoverishment. In the manic state, the person’s “moral brakes” are out of control. This can lead to oversexualized or aggressive behaviour, causing irreparable damage to him and his family. Therefore, in most of the cases, the patients require hospitalization. The medication used in the acute phase must be administered quickly and in sufficient dosage. The most frequent medication used in the acute phase is a combination of atypical antipsychotics (Quetiapine, Olanzapine, and Risperidone) and a mood stabilizer, preferably Valproic acid.
Medication for Bipolar Depression
In the depressive phase, the problems are different. The patient suffers from lack of energy, low mood, sleeplessness, and often develops suicidal ideation. Depressive episodes in bipolar disorder are far more common than mania and have a more detrimental effect on patient’s lives.
In some patients, mood stabilizers may be sufficient to modulate the depressed mood. However, the standard treatment for bipolar depression is the combination of an antidepressant and a mood stabilizer. The mood-stabilizing medication improves mood, social interactions, and the patient’s level of functioning. The sole use of antidepressants in bipolar depression carries the risk of transitioning into a hypomanic or manic phase. The mood stabilizer of choice in the treatment of bipolar depression is lithium because of its antisuicidal properties.
Only one of the atypical antipsychotics, Quetiapine, is worth mentioning, as it can achieve good antidepressant effects at doses of 300-600 mg in bipolar depression.
Maintenance Therapy for Bipolar Disorder
Patients suffering from BP, which is a lifelong and recurrent illness, need long-term treatment to maintain control of symptoms. Therefore, psychiatrists should closely monitor the mental health of their patients and adjust medication accordingly. Relapse prevention begins once the individual’s mood has returned to a normal and stable level. Its purpose is to reduce the long-term risk of future acute episodes.
In the phase of the maintenance therapy, the patient typically feels much better or is even symptom-free, which often leads to a decrease in motivation to take daily medication. It is important to emphasize to the patient that discontinuing the medication causes a significant risk of relapse. Psychiatrists should address their patients’ concerns openly, thereby improving their insight and coping skills.
The duration of relapse prevention depends on the number of previous episodes. If a person has experienced three or more episodes within a five-year period, long-term maintenance treatment with medication is generally recommended to help prevent further episodes.
The main therapeutic obstacle in the treatment of bipolar disorder lies in convincing the patient to comply with the recommended therapy, particularly the regular intake of prescribed medication.
Antipsychotics for Bipolar Disorder
Antipsychotics such as aripiprazole, lurasidone, olanzapine, quetiapine, risperidone, and ziprasidone are well established in the treatment of acute manic phases. They are mostly used in combination with a mood stabilizer. Among them, only quetiapine has approval for relapse prevention and is effective even in bipolar depression. Evidence suggests that antipsychotics may also enhance the effects of mood stabilizers after the acute phase.
Although all these medications can cause extrapyramidal side effects and akathisia, the risk is lower with more sedating drugs like quetiapine and olanzapine. Long-term side effects may include significant weight gain and the development of metabolic syndrome, which involves weight gain, excess abdominal fat, insulin resistance, and dyslipidemia. The risk of these metabolic effects is lower with less sedating antipsychotics like lurasidone, ziprasidone, and aripiprazole.
Mood stabilizers
This group of medications is used to treat bipolar disorder, either alone or in combination with antipsychotics. They can be used throughout all treatment phases, stabilizing mood swings during both manic and depressive episodes. Some mood stabilizers are effective only for the treatment of mania, and others are for bipolar depression. Few of them protect the patients “on both sides”: from mania and from depression. They stabilize the prevailing mood without inducing opposite episodes, which is crucial in preventing relapse even during stable phases. The most frequently applied mood stabilizers are lithium, valproate, lamotrigine, and carbamazepine.
Anticonvulsants with Mood Stabilizing Effect
Anticonvulsants that act as mood stabilizers, particularly valproate and carbamazepine, are commonly used to treat acute mania and mixed states (mania and depression). Lamotrigine is effective for mood swings and depression. While the exact mechanism of anticonvulsants in bipolar disorders remains unclear, it may involve gamma-aminobutyric acid (GABA) pathways and G-protein signaling systems. Compared to lithium, their primary advantages are a wider therapeutic range.
Valproate
The dosage of valproate depends on target serum levels and can be adjusted based on weight-based protocols to achieve quicker symptom improvement. Common side effects include nausea, headaches, sedation, dizziness, and weight gain.
Lamotrigine
The dose of lamotrigine should be increased gradually to avoid the risk of skin rash. Patients under lamotrigine should report any new skin rash, hives, fever, swollen glands, mouth or eye sores, or swelling of the lips or tongue.
Carbamazepine
Also, carbamazepine requires gradual dose increases to reach therapeutic serum levels. Starting with a higher dose carries risks of nausea, dizziness, and sedation, with severe but rare side effects such as agranulocytosis.
Lithium for Bipolar Disorder
Lithium stabilizes bipolar mood swings. Patients with a family history of typical bipolar disorders are more likely to respond positively to lithium.
Lithium carbonate is usually titrated based on blood levels, tolerability, and response. Higher maintenance blood levels provide better protection against manic episodes (though not depressive episodes) but are associated with more side effects. Adolescents with excellent kidney function typically require higher doses, while older patients require lower doses.
The most common mild acute side effects include fine tremor, nausea, diarrhea, polyuria, polydipsia, and weight gain (partly due to the consumption of calorie-rich drinks). These effects are generally temporary and often respond to a slight dose reduction, splitting the dose into smaller portions (e.g., three times daily), or using sustained-release formulations. Once the dosage is stabilized, the entire dose should be taken after the evening meal, as this once-daily regimen can improve adherence. Lithium blood levels should be monitored every six months and after any dose adjustments.
Benzodiazepines
Benzodiazepines are drugs with sedative and anxiolytic effects. Their mechanism of action involves binding to the GABA-A receptor. By enhancing the effects of GABA, they reduce activity in certain areas of the central nervous system, leading to decreased responses to emotional and psychological stimuli. While individual benzodiazepines differ in terms of pharmacokinetics, their fundamental pharmacodynamics remain similar and are primarily determined by dosage.
Since the introduction of the first benzodiazepine, chlordiazepoxide (Librium), in the 1960s, numerous substances with varying pharmacological profiles have been developed. Just three years after chlordiazepoxide was launched, diazepam (Valium) followed.
Benzodiazepines are important in cases of severe manic psychosis, where immediate patient safety and behavioral management are at risk. Achieving behavioral control requires a sedative second-generation antipsychotic, initially combined with a benzodiazepine like lorazepam or clonazepam.
Antidepressants for Bipolar Depression
The guidelines do not recommend using an antidepressant as monotherapy for acute bipolar depression. Similarly, there is no recommendation for a specific medication.
During the course of bipolar depression, symptoms can relatively quickly shift to a manic or mixed episode. It is not proven what role the use of antidepressants plays in such a “switch.”
Specific antidepressants (e.g., selective serotonin reuptake inhibitors, SSRIs) are sometimes used for severe depression, but their effectiveness is controversial. They are generally not recommended as monotherapy for bipolar depression, although there is evidence suggesting the use of SSRIs (selective serotonin reuptake inhibitors) like fluoxetine, paroxetine, or sertraline.
The other option could be the use of an atypical antidepressant belonging to norepinephrine–dopamine reuptake inhibitor (NDRI), bupropion. A number of smaller studies indicate that tranylcypromine might be more effective in treating bipolar depression than other antidepressants. A higher risk appears to be associated with treatment using tricyclic antidepressants and venlafaxine.
Due to the risk of switching to a manic episode, antidepressants are most commonly used in combination with a mood stabilizer or an antipsychotic in the treatment of bipolar depression.
Medication for Bipolar Disorder in Bullet Points
• Motivation: Medication needs to be thoroughly discussed with the patient. Many people with bipolar disorder struggle to accept that they need to take medication long-term or even permanently. Comprehensive conversations can help build acceptance and improve compliance, which leads to treatment success.
• Individualized therapy adjustment: It may take some time to find the right medication. Individual symptoms and side effects need to be considered in the medication treatment plan.
• Regular monitoring: The effect of maintenance and prophylactic phases needs to be regularly monitored.
• Acute mania in bipolar disorder: mood stabilizers such as lithium, valproic acid, carbamazepine, and lamotrigine, as well as atypical antipsychotics such as olanzapine, risperidone, quetiapine, ziprasidone, and aripiprazole, are used. Combinations of both are usually more effective.
• Acute depression in bipolar disorder: Only combinations of mood stabilizers and antidepressants make sense, and antidepressants should not be used alone in bipolar disorder. Quetiapine is an alternative to monotherapy.
Medication for Bipolar Disorder. Final Thoughts
Medication is one of the most important parts of bipolar disorder treatment. Without the right medication, it is very difficult to stabilize either manic or depressive episodes. Even during stable periods, there is still a risk of relapse if bipolar disorder is left untreated.
The choice of medication always depends on the individual symptoms and on whether manic or depressive phases are more dominant. Because of its complexity, medication and treatment of bipolar disorder should always be supervised by an experienced psychiatrist.
Antipsychotics and mood stabilizers are the first choices during manic episodes. These medicines help reduce excessive energy, agitation, impulsive behavior, and feelings of extreme euphoria. They calm the mind and protect patients from risky decisions or loss of control.
In depressive phases, antidepressants can be used; however, in bipolar disorder, antidepressants are usually combined with mood stabilizers or atypical antipsychotics. This is important because antidepressants alone can trigger a manic episode.
Mixed episodes can be especially difficult to treat because symptoms of depression and mania appear at the same time. In these cases, several medications may need to be taken together.
Preventing relapses is another key goal of treatment. Mood stabilizers and some antiepileptic medications can lower the risk of future depressive or manic episodes and help patients stay emotionally stable over the long term.
Read More About Bipolar Disorder
- Treatment for Bipolar Disorder
- Symptoms of Bipolar Disorder
- Diagnosis of Bipolar Disorder
- Self-Test for Bipolar Disorder
- Psychiatrist for Bipolar Disorder
- Bipolar Disorder in Pregnancy
- Psychotherapy for Bipolar Disorder
- Causes of Bipolar Disorder
- Bipolar I vs Bipolar II Disorder
- What is Rapid Cycling?
- Bipolar Disorder and Sleep
- Living with Bipolar Disorder
- Relationships, Family, Everyday Life with BD
- Long Term Recovery & Quality of Life with BD
- Family Support in Bipolar Disorder
- What is Mania and Hypomania?
- Cyclothymic Disorder
- History of Bipolar Disorder
- CANMAT Guidelines for Bipolar Disorder
- Mood Stabilizers for Bipolar Disorder
- Lithium for Bipolar Disorder
Medically reviewed by Dr. Gregor Kowal

DR. GREGOR KOWAL
Dr. Gregor Kowal is a German-certified consultant in Psychiatry and Psychotherapy. Since 2010, Dr. Kowal has been the Medical Director of CHMC, a psychiatric clinic located in Dubai. Dr. Kowal graduated from the prestigious University of Heidelberg. After completing his specialty training, he held leadership and teaching positions, serving as Head of Department and later as Medical Director at renowned psychiatric hospitals across Germany. In addition to his expertise in psychiatry, Dr. Kowal is trained as a psychotherapist with a foundation in psychoanalytical psychotherapy.

